
Research Article | DOI: https://doi.org/10.31579/2578-8868/168
*Corresponding Author: Atroune L, Mustapha Bacha Hospital, Department of Neurosurgery, Algiers, Algeria
Citation: Atroune L., Bennaleg S.,, Habchi N., Bouaita K., and Djaafer M., (2021) PITUITARY ADENOMA IN THE ELDERLY J. Neuroscience and Neurological Surgery. 8(5); DOI:10.31579/2578-8868/168
Copyright: © 2021 Atroune L, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 26 February 2021 | Accepted: 03 March 2021 | Published: 10 March 2021
Keywords: transnasal- trans; sphenoidal; elderly; hypopituitarism
Given advances and wide availability of neuroimaging coupled with longer life span, higher numbers of elderly patients with pituitary adenomas are being seen who are potential surgical or medical therapy candidates.
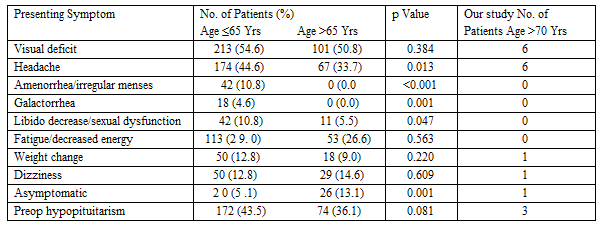
Our study concerns 07 cases of Pituitary adenoma in patients aged more than 70 years old, collected in Mustapha Pasha’s neurosurgery department in Algiers for a period of 18 years (from 2000 to 2018). Pituitary adenoma is not considered a disease of advanced age; its incidence is rated around 3–4%. The average age of patients was 72 years old, slightly more common in females and represents 60% of the cases. The average duration of symptoms before diagnosis is 2 and half years. The clinical signs were dominated by visual deterioration, and in a lesser degree a hypopituitarism.
Neuro-imaging (CT scan/ MRI) are the key exams. MRI is important especially in the development of surgical planning. Collected radiological data reported the presence of macro adenoma with supra sellar extension in the majority of our cases;
The surgical approach was transnasal- Transsphenoidal in all patients. The evolution was satisfactory for the majority of patients. However, complications were noted. We deplore the death of a patient presented with meningitis. Patients over age 70 with pituitary tumors and indications for surgery should be considered surgical candidates for transsphenoidalsurgery given the low risks of this procedure.
Pituitary adenomas (PAs) are common benign intra-cranial neoplasms, with an estimated prevalence of 16.7% in the general population. [3,4]. Non functioning PAs (NFPAs) are a type of PA without clinical evidence of excess hormone secretion, and, due to their silent nature, patients present with symptoms related to mass effect, such as visual disturbances. [5].
Life expectancy has increased over the past century; causing a shift in the demographic distribution in developed countries toward older age groups. [6]. Also, skull base surgery in geriatric patients has been becoming increasingly common, particularly with the emergent use of the endoscopic trans-phenoidal (TNS) approach [7].
Elderly patients account for up to 14% of all patients diagnosed with pituitary tumors, with most lesions being NFPAs. [8,9].
While several studies have shown the relative safety of transsphenoidal surgery for elderly patients with symptomatic pituitary adenomas, the complication rates reported in the literature with progressive age remain significant and cautionary [10,11,12].
According to the latest guidelines, TNS is recommended in elderly patients with NFPAs associated with visual disturbances [13,14], whereas the indication for surgery in individuals without evidence of visual impairment is still a matter of debate, given the slow growth of PAs and the increase in age-related anesthetic and surgical risk ]13,15,16,17].
The treatment of choice mainly depends on the local extension of the tumor, clinical presentation, tumor size and configuration, and overall patient health [18, 19, 9, 20, 21]. But no consensus guidelines are available in elderly patients who often present with a greater number of medical comorbidities and less physiological reserve, predisposing them to an increased rate of surgical complications. In order to critically review our experience with the treatment of pituitary adenomas in the elderly, we have retrospectively analyzed the surgical treatment, outcome of 07 patients with pituitary tumors, who were more than 70 years of age at the time of surgery.
The study included 07 patients older than 70 years, who were diagnosed and treated or pituitary adenomas between the year 2000 and 2018.
In all patients complete hormonal screening was obtained and the visual acuity and visual fields were examined pre- and postoperatively. Immunocytochemical studies with polyclonal anti-GH, anti-PRL, anti-FSH, anti-LH, anti-TSH and anti-ACTH antibodies were performed. The anesthesiological risks were staged according to the American Society of Anesthesiologists (ASA) scale. Surgical indications were the presence of neurological signs or symptoms related to the tumor mass at presentation, a rapid growth of the lesion and a hormonally active pituitary adenoma.
Tumor size and extension were evaluated with the Hardy classification. Neurological and endocrinological examinations were performed before and after the operation and at 6 months-intervals after surgery. Findings from patients, clinical records, radiological examinations and operative reports were recorded.
The surgical procedures were performed by a dedicated team in our Neurosurgery department. All patients underwent a transseptal transsphenoidal microscopic approach according to the modified Hardy technique. Postoperatively the patients were transferred the ICU, with special attention to heart and circulation homeostasis and fluid-electrolyte balance and Monitoring of hourly diuresis.
Follow-up included a yearly clinical examination and basal hormonal assessment of pituitary function. Neuroradiological imaging and endocrinological follow-up was performed 3 months after surgery.
The study included 07 patients older than 70 years, affected by pituitary adenomas (4 non-functioning pituitary adenomas, 2 GH secreting adenomas, 1 ACTH-secreting adenoma). The average age of the patients was 72 years. 3 patients were men and 4 were women; Clinical presentation reflected tumour-related mass effect in 6 patients, with headaches present in 5 patients and visual field deficits in 6 patients. 01 patient presented sudden headache and worsening vision.
Tumor size and extension were evaluated with the Hardy classification: One case was considered an intrasellar adenoma, 05 cases an enclosed adenoma with little suprasellar extension. The rest of the cases appeared as adenomas with marked suprasellar extension.
Patients included in the study presented with a high incidence of comorbidities, cardiovascular diseases being the most frequent. Before surgery all the patients were classified following the American Society of Anaesthesiologists physical status classification system. An ASA score of 1 was assigned to 1 patient. The ASA score was 2 in 4 patients, ASA 3 in 1, and ASA 4 in 1 case.

All patients underwent a transseptal-transsphenoidal microscopic approach; appropriate intraoperative and postoperative glucocorticoid supplementation was administered to all patients. Two patients complained of postoperative permanent diabetes insipidus, no post-operative CSF-leak. One patient died after surgery.
As far as the anterior pituitary function is concerned, no patient recovered a pre-existent pituitary deficit. An additional hormonal deficit was observed in 1 patient. Finally, a significant visual field improvement was demonstrated in 05 of our patients with preoperative visual deficits, while headache resolved in all patients with this disturbance.
The most common endocrine changes of healthy aging are declines in GH and IGF-I, ovarian steroids in postmenopausal women, testosterone (T) in men and DHEA. Aging is associated with an increased frequency of pituitary tumors, detected incidentally in 10%–25% of hypothalamic-pituitary MRIs performed in older persons. [22]
In this study, we present our experience with transsphenoidal surgery (TSS) between 2000 and 2018 in 07 patients with pituitary adenomas, aged more than70 years at the time of surgery. From this 07 elderly patients, NFPAs represented 57, 18% of the whole serie, with GH- secreting adenomas accounting for 2 and 28, 57% and 01 adrenocorticotrophin (ACTH)- secreting adenomas, respectively. Similar figures have been reported by others, with NFPAs representing 55–84% of all cases, followed by GH- (9–27%), PRL- (4.5–10%) and adrenocorticotrophin (ACTH)- (0–6%) secreting adenomas, respectively [22, 23, 24, 25, 26]. Noteworthy is that some studies suggest that the incidence of gonadotroph adenomas, usually included in the NFPA group, tends to increase with age and to be more frequently diagnosed above 60 years, especially in men [27, 28].
There was a clear male predominance, which also was thereby probably implying that there is a later onset of symptoms in men harboring clinical non functioning macroademomas observed in previous studies.
Given the increase in life expectancy and the expansion in use of MRI and CT imaging, it is presumed that the prevalence of diagnosed PAs in the elderly population will grow [7]. Previous studies have confirmed this trend, with a steady increase in the proportion of PA cases being in elderly patients over the past 3 decades [18, 9, 29 and 30].
The growth of PAs is generally slow in elderly and about 25% of asymptomatic macro adenomas may increase in size over 5 years of follow-up [31,32]. This can be supported by the low rates of cell proliferation commonly reported in this age group [33]. An age-related decrease in cell proliferation has been observed in NFPAs(34) and in GH-secreting tumours [14], the latter being mostly intrasellar in the elderly [23, 24, 35].
Moreover, the diagnosis of NFPAs in the elderly is frequently late, due to the low specificity of clinical symptoms and signs of pituitary diseases in this clinical setting (13,36,37,38). The most common symptom was the visual impairment, especially loss of acuity and bitemporal hemianopsia due to suprasellar extension of adenomas. Dynamic endocrinological testings were not routinely performed, so that the incidence of subclinical pituitary insufficiency could be higher, as reported in other studies [21].
The clinical presentation of a pituitary adenoma in the elderly can be very atypical. Physiological endocrine changes due to age, frequent co-morbidities, visual field impairment by senile degeneration can confuse or delay the diagnosis, which has been supported by series published in the literature [23]. Other explanations are also mentioned, including less tumor aggressiveness at this age in connection with lower GH and IGF1 levels than in young adults [24], in fact elderly subjects are more likely to have micro adenomas than young patients with this hypothesis. In addition, age-related variations in endocrine and paracrine factors, such as sex hormones, metabolic factors or tumor vascularity may be responsible for this difference [39]. It has also been reported in the literature that pituitary insufficiency is more likely in young patients [39]. A relationship between the size of the tumor and the degree of pituitary insufficiency has been suggested [25].
Despite an increased anesthesiological risk present in most of the patients, we only lost one patient and one severe anesthesiological complication was observed (diabetes insipidus), and one with cerebrospinal fluid leak [40].
The post-operative hospitalization period for the whole series was about 15 days, similar to those reported by previous studies with an average LOS ranging from 3–18 days [41, 42].
Previous studies reporting visual symptom improvement of 71%–100% after surgery in these patient demographics, the same was observed in all of the patients, supporting evidence that curative TSS is the treatment of choice for NFPAs causing visual failure [9, 43, 44 and 45].
TSS carries known risks of pituitary stalk perturbation leading to syndrome of inappropriate antidiuretic hormone secretion (SIADH) or DI causing hyponatremia or hypernatremia, respectively (48,49). Studies evaluating clinical outcomes in elderly patients undergoing TSS have found a similar incidence of DI in this age group, with permanent DI rates as high as 5% [9, 10, 50, 51, 52, 20 and 29].
In this group, anterior pituitary function worsened in 1 of patient and two presented with hyponatremia while pre-operative hypopituitarism remained unchanged in most. no significant improvement of impaired pituitary function was observed similar to some studies have suggested that elderly adenoma patients are less likely to show gland function improvement and have higher rates of new hypopituitarism, however data is limited [53] Recent studies addressing pituitary adenoma surgery in the elderly are summarized in Table 2. [46, 47]

In literature, it was relatively clear that postoperative DI after TSS reflects some degree of stalk injury, the mechanisms of hyponatremia after TSS are less clear but may reflect abnormal release of ADH or brain natriuretic peptide causing SIADH or cerebral salt wasting [54,55]. Hyponatremia is favoured by adrenal failure and age-related changes in vasopressin secretion. It is possible that age-related structural changes in the pituitary gland, such as increased interstitial and perivascular fibrosis, may confer the age-related protection against postoperative DI that was identified in previous studies [56, 21]. In contrast, age-related predispositions to electrolyte perturbations due to medications that elderly patients commonly take or age-related changes in the release threshold of natriuretic factors may contribute to the age related increase in hyponatremia we and previous studies has identified [47,21].
The retrospective nature of our study brings the usual limitations of a retrospective analysis like the missing cohort of our patients followed without surgery due to lack of an electronic medical record. In particular, some inconsistencies in the frequency of outpatient sodium checks could affect our findings about hyponatremia. Also long term tumor control of endocrine-inactive adenomas and biochemical remission in endocrine-active adenomas for some patients was not analyzed. Thus, it is likely that with longer follow-up some patients will require additional treatments such as radiosurgery, hormonal therapies and possibly repeat surgery.
TSS alone was performed in all our patients with total or subtotal resection of the adenoma. There was no regular follow-up approaching, so we weren’t able to conclude the overall rate of recurrence. The rate of regrowth in NFPAs is known to be mainly influenced by the quality of surgical resection [21]. Previous studies showed that pseudocapsular resection was not associated with the deterioration of the pituitary functions in elderly patients with NFPA; moreover, pseudocapsular resection might reduce the risk of postoperative hemorrhage (58).
According to recent series [21, 46], and to our data, even if obtained in a small number of patients, surgery could be safely performed in elderly.
In conclusion, our study indicates that TSS can be safely performed for patients older than 70 years. In the majority of cases it is able to improve the visual defects, and may represent the only therapy for patients with NFPA. The timing of surgical treatment seems to be an important determinant of postsurgical outcomes, especially when performed by a multidisciplinary team with a specific experience in pituitary diseases; we only need to keep in mind that the primary goal is the minimum mortality or relevant adjunctive morbidity.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
